Newest insights into depression and suicidality amongst healthcare workers
The completed suicides of the pre-Pandemic (2019) to provisional 2020 have been studied and are shown below according to National Center for Health Statistics. Based on this data, it appears that at least for the year 2020, there was not an increase in overall completed suicides in the general population.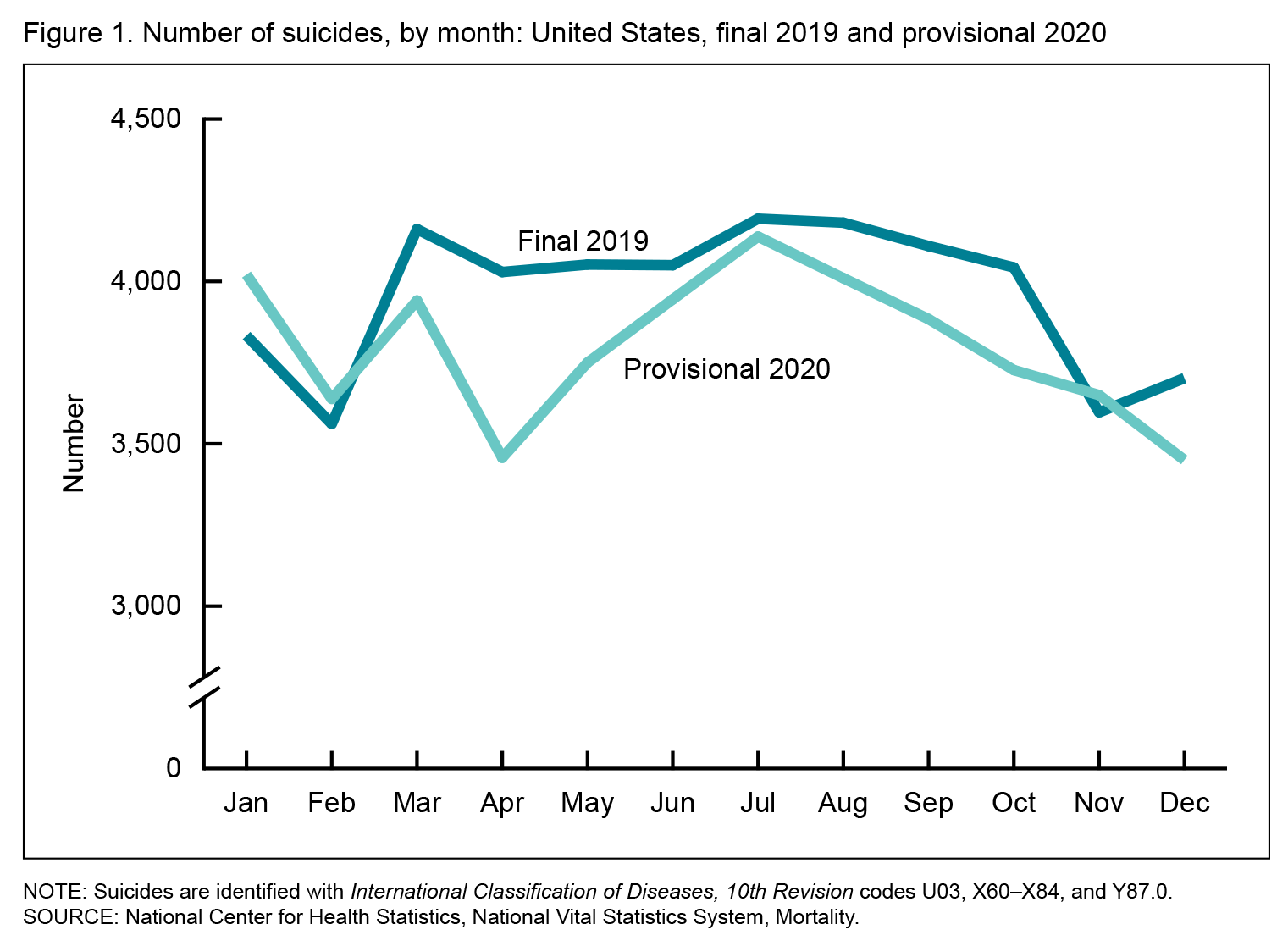
That being said, an area often overlooked, is depression and suicidality amongst healthcare workers. According to Centers for Disease Control and Prevention (CDC), Healthcare workers have historically been at disproportionate risk of suicide, due to a variety of factors, including:
- difficult working conditions, such as long work hours, rotating and irregular shifts,
- emotionally difficult situations with patients and patient’s family members,
- risk for exposure to infectious diseases and other hazards on the job, including workplace violence,
- routine exposure to human suffering and death, and
- access to lethal means such as medications and knowledge about using them.
According to American Foundation for Suicide Prevention, Physicians have higher rates of burnout, depressive symptoms and suicide risk than the general population (1.4 x’s for general male and 2.27x’s for general female). Physicians report several barriers to seeking mental health care, including time constraints, hesitancy to draw attention to self-perceived weakness, and concerns about reputation and confidentiality. Physicians who proactively address their mental health are better able to optimally care for patients and sustain their resilience in the face of stress.
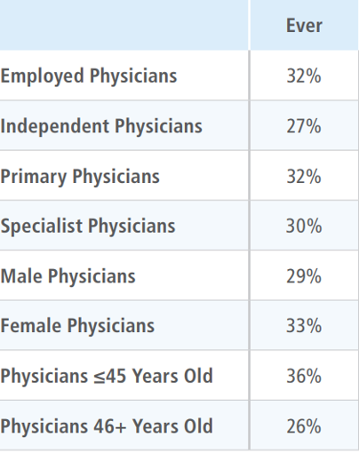 The Physicians Foundation in 2021 released the results of a national survey, which finds that more than half (55%) of physicians know a physician who has considered, attempted or died by suicide in their career. When asking if physicians had personal knowledge of a physician who considered suicide, the results are shown at left.
The Physicians Foundation in 2021 released the results of a national survey, which finds that more than half (55%) of physicians know a physician who has considered, attempted or died by suicide in their career. When asking if physicians had personal knowledge of a physician who considered suicide, the results are shown at left.
According to American Foundation for Suicide Prevention, health care professionals who are proactive about their own health — both physical and mental — protect their ability to maintain optimal, safe patient care. Real and perceived barriers lead many health care professionals to avoid addressing their own mental health needs all too often. An unprecedented number of health care professionals experience burnout, depression and other forms of distress, and are at in increased risk for suicide as compared to the general population.
Columbia-Suicide Severity Rating Scale (C-SSRS) is a questionnaire used for suicide assessment, developed by multiple institutions, including Columbia University. Several versions of the C-CCRS have been developed for clinical practice. The C-SSRS Risk Assessment is intended to help establish a person’s immediate risk of suicide and is used in acute care settings.
National Suicide Hotline Improvement Act Proposed a 3-digit number for mental health and suicide crisis vs. the current 1-800-273-TALK. The three-digit number makes the National Suicide Prevention Lifeline easier to remember and therefore more accessible. It also Relieves overburdened 911 dispatchers by linking with more appropriate care when it’s needed the most. The new three-digit number places calling for mental health crises on the same level as calling 911 for medical crisis. As such, 988 has been designated as the new three-digit dialing code that will route callers to the: National Suicide Prevention Lifeline. While some areas may be currently able to connect to the Lifeline by dialing 988, this dialing code will be available to everyone across the United States starting on July 16, 2022.
Last review date: June 6, 2022